Anterior Cruciate Ligament Tears in Gymnastics

Anterior cruciate ligament
The ACL Consists Of 2 Bundles, AM & PL Bundles
- The 2 ACL bundles are named according to their tibia attachment with the AM bundle inserting antero-medially and the PL bundle inserting posterolaterally.
- On the femoral side, the AM bundle originates more proximally than does the PL bundle.
- The AM bundle tightens in flexion while the PL bundle relaxes.
- The PL bundle tightens in extension while the AM bundle relaxes.
- AM and PL bundles have maximal shortening peak at 30° of knee flexion.
- The AM bundle gives maximal rotation stability at 60°-90° knee flexion.
- The PL bundle gives maximal rotation stability at 15°-20° knee flexion.



Examination
ACL Instability Tests:
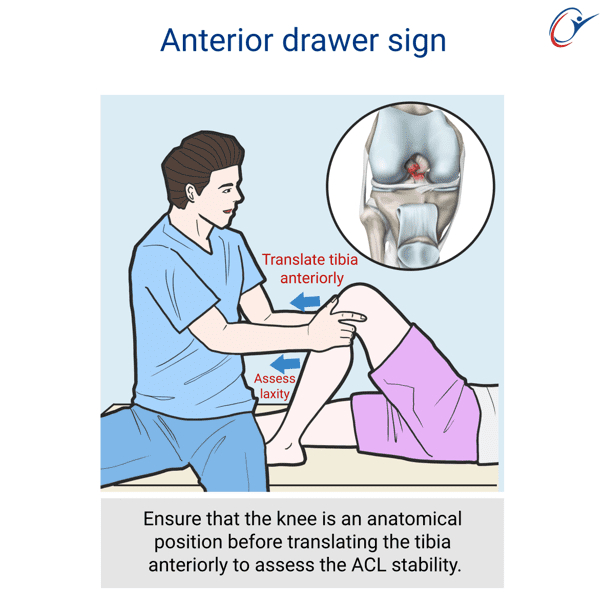
- Anterior drawer sign
- Lachman test
- Pivot test
Lachman test
Hold patient’s leg with knee flexion to 30 degrees.
With knee flexion at 30 degrees, translate tibia anteriorly.
Positive test with anterior tibia translation

Drawer test
With tibia in anatomical position with knee flexion at 90 degrees, the tibia is translated anteriorly to assess for ACL instability and translated posteriorly to assess for PCL instability.
Video: Combined ACL & PCL instability. The knee is assessment & test performed from anatomical position for increased anterior & posterior tibia translation.
Pivot test
With leg extended internally rotate the tibia and apply a valgus knee force while flexing the knee joint. At 20-30 degrees of knee flexion the reducing lateral tibia plateau will produce clunk as it reduces to an anatomical position.

Overview of ACL reconstruction surgery principles
Video: ACL Reconstruction
Surgery Technique

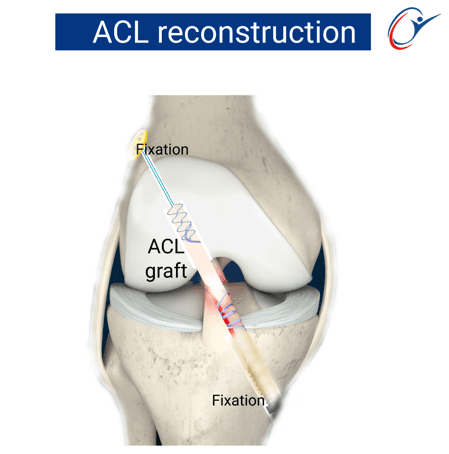
Anterior cruciate ligament reconstruction
Anterior cruciate ligament reconstruction surgery principles include anatomical ACL reconstruction using allograft or autograft. Concomitant injuries are addressed simultaneously to ensure knee stability with a decreased risk of graft failure and also ensuring return to play at previous level of functioning.
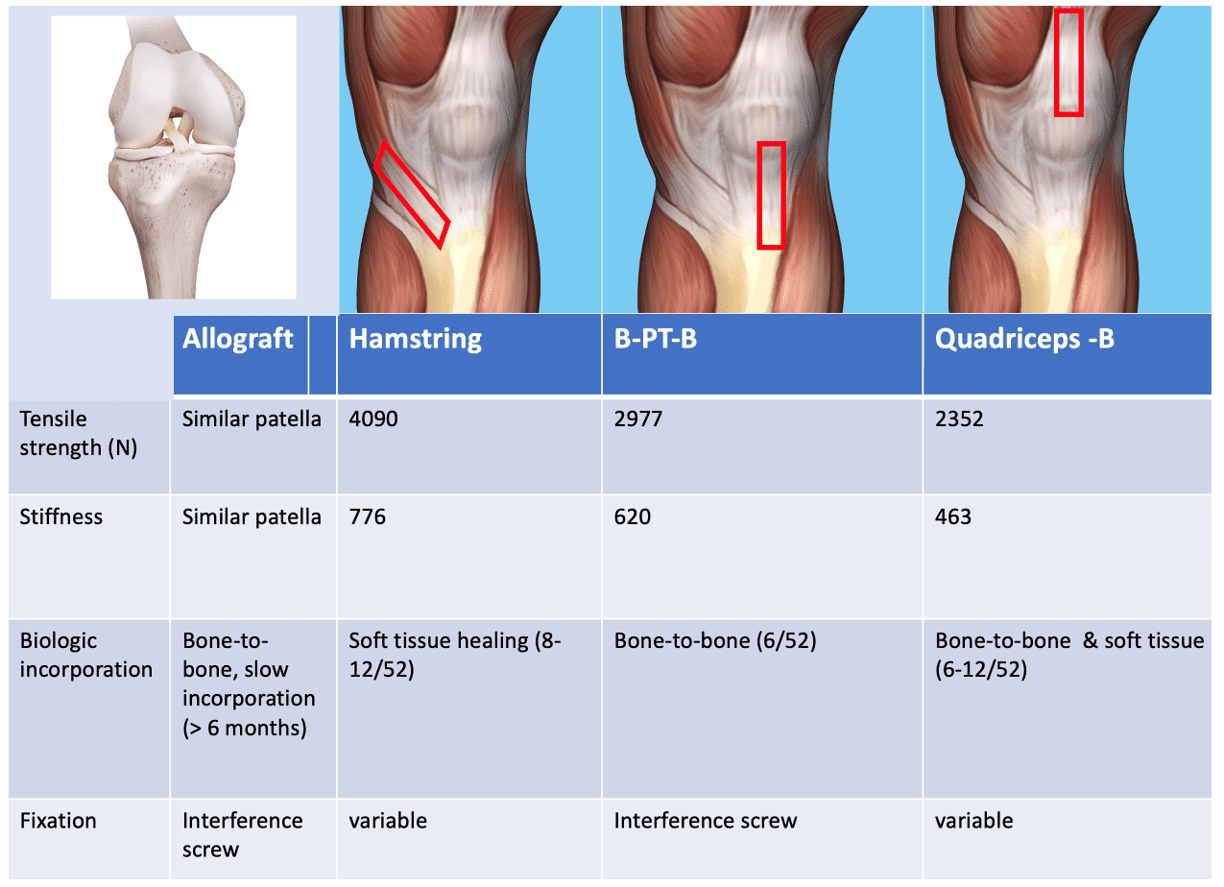
ACL graft options
Graft options include autograft or allograft.
Autograft include:
- Hamstring
- Quadriceps patellar bone
- Bone patellar tendon bone
Graft complications
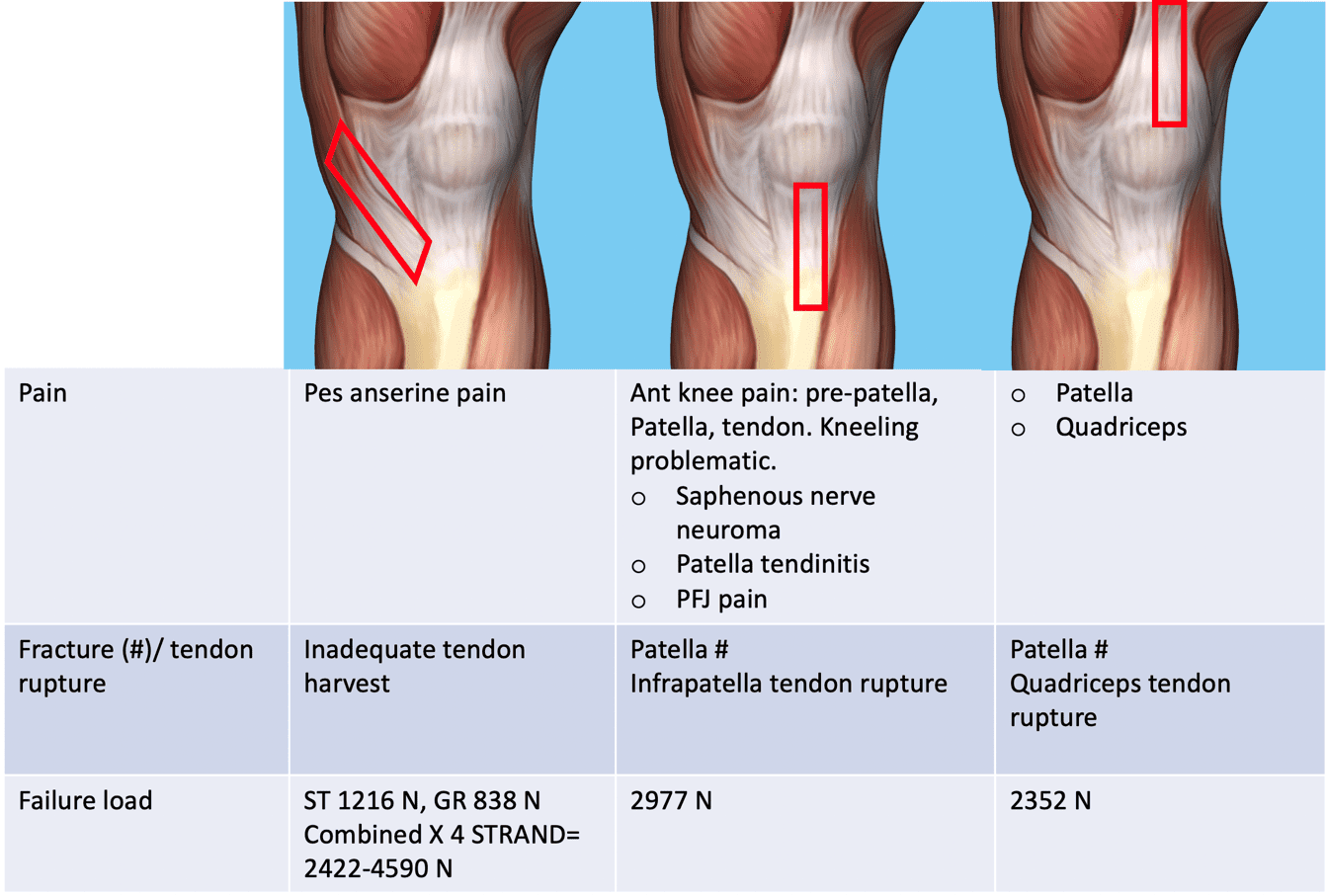
Graft preparation
Harvest autograft or use allograft.
Suture fixation of the graft ends.
Size graft to determine the drill size of the femur or tibia tunnels.

Suture Ends Of Graft

Size Graft To Determine Tunnel Diameter
Preparation of femur tunnel
Arthroscopic view of femur ACL insertion site.
Drill the lead K-wire at femur insertion site.
Drill cannulated drill over the K-wire.
Size length of tunnel.
When using Smith & Nephew endobutton, the graft diameter tunnel length require an extra 10mm of drill length to allow flipping of the endobutton when the graft is passed through the femur tunnel.

Drill wire through ACL femoral attachment site
Use cannulated drill bit drilling over wire
Measure femur tunnel length

Drill diameter of graft size, preferably 8mm graft diameter
Pull loop suture and keep in situ
Prepare Tibia tunnel
Preparation of tibia tunnel
Use tibia jig and drill the tibia tunnel.
Have appropriate tunnel length and angle of tunnel.
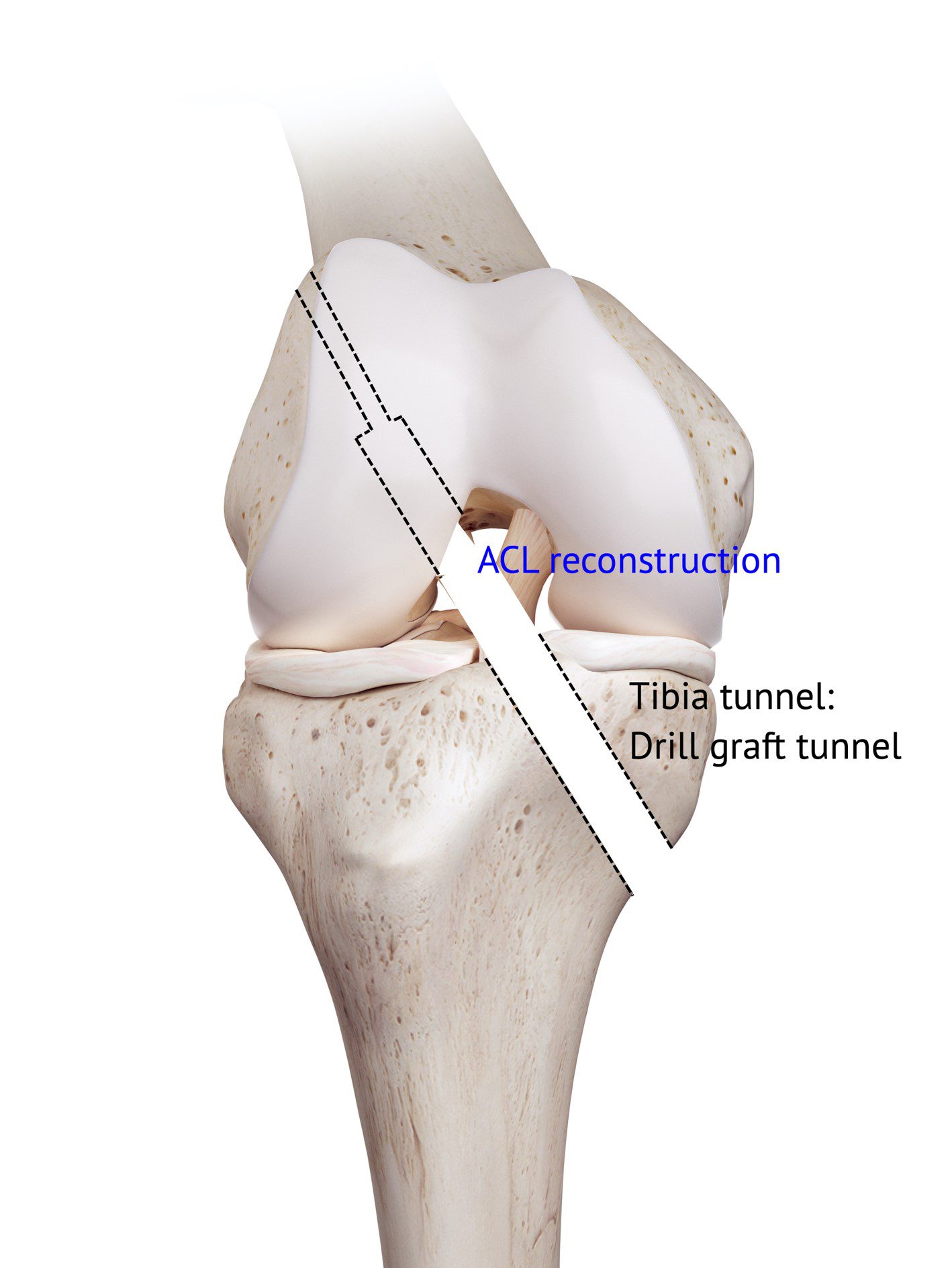
Drill tibia tunnel to graft diameter
Passing of ACL graft through the prepared tunnels
Pull loop suture from femoral tunnel through tibia drill hole.
Pull the endobutton sutures (attached graft to endobutton) through the femur tunnel.
Flip endobutton and toggle to ensure flipped endobutton has flipped.


Fixation of graft to tibia
Pull graft at tibia end and apply inline traction to the graft while securing it with screw fixation.
ACL graft fixation at 30° knee flexion with screw fixation.
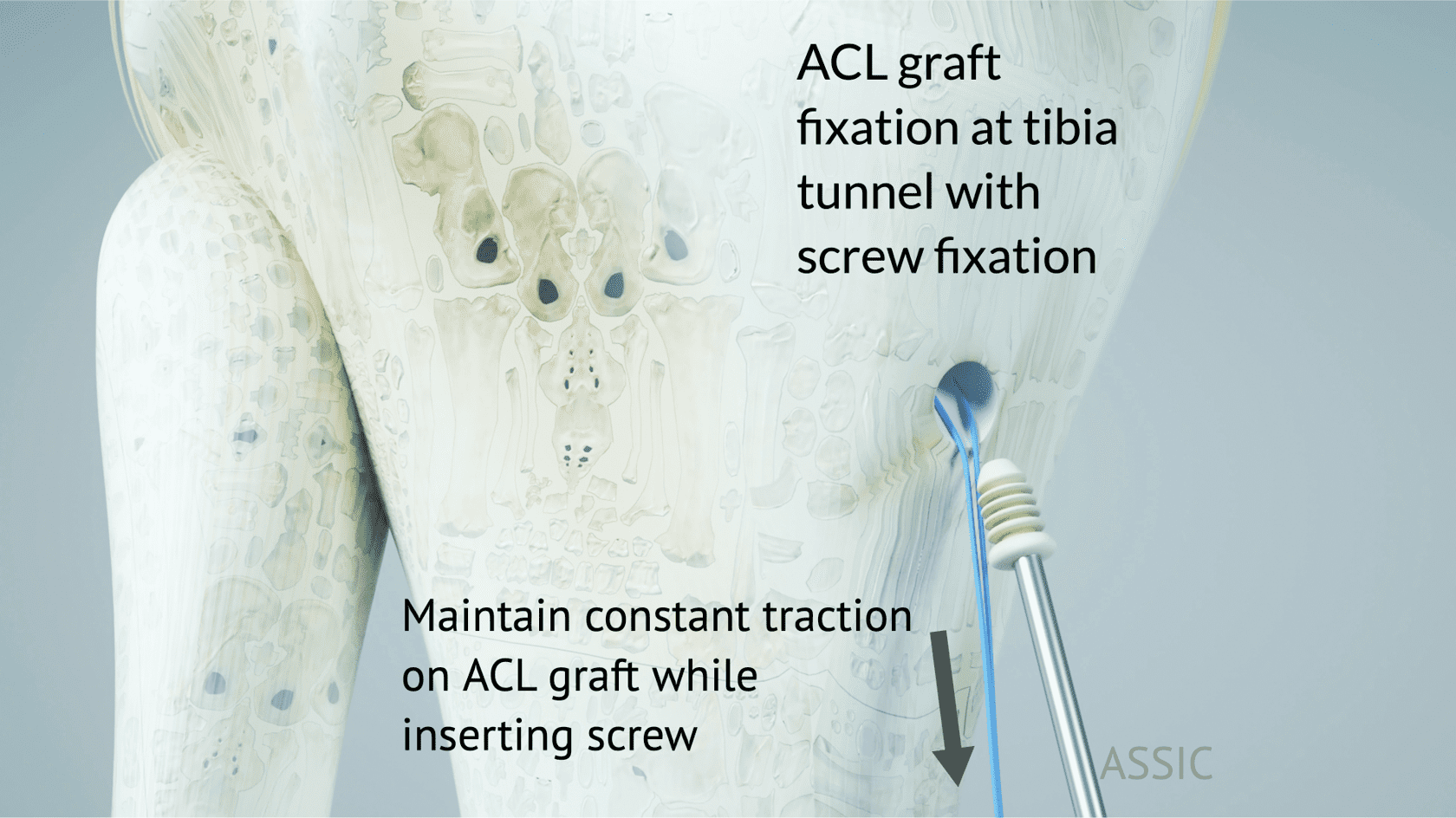
Tension ACL graft and insert tibia screw
References
- Markolf KL, Feeley BT, Jackson SR, McAllister DR: Where should the femoral tunnel of a posterior cruciate ligament reconstruction be placed to best restore anteroposterior laxity and ligament forces? Am J Sports Med 2006; 34:604-611.
- Matava M J, Ellis E, Gruber B. Surgical Treatment of Posterior Cruciate Ligament Tears: An Evolving Technique. J Am Acad Orthop Surg 2009;17: 435-446.
- Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS: Two-bundle posterior cruciate ligament reconstruction: An in vitro analysis of graft placement and tension. Am J Sports Med 2000;28:833-845.
- Eakin CL, Cannon WDJ. Arthrometric evaluation of posterior cruciate ligament injuries. Am J Sports Med. 1998;26:96-102.
- Petrie RS, Harner CD. Evaluation and management of the posterior cruciate injured knee. Oper Tech Sports Med. 1999;7:93-103.
- Harner CD, Baek GH, Vogrin TM, Carlin GJ, Kashwaguchi S, Woo SL: Quantitative analysis of human cruciate ligament insertions. Arthroscopy 1999; 15:741-749.
- Takahashi M, Matsubara T, Doi M, Suzuki D, Nagano A: Anatomical study of the femoral and tibial insertions of the anterolateral and posteromedial bundles of the human posterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 2006;14:1055-1059.
- Edwards A, Bull AM, Amis AA: The attachments of the fiber bundles of the posterior cruciate ligament: An anatomic study. Arthroscopy 2007;23:284-290.
Contributor
Dr M Y Hassan